|
|
-----------------------------------
Departments: Molecular Biology and Genetics Preimplantation Genetic Screening
|
Molecular Biology and Genetics Department1. Genetic predisposition to recurrent pregnancy loss, clotting disorders and venous thrombosis in both genders: 2. Male infertility:
Genetic predisposition to recurrent pregnancy loss, clotting disorders and venous thrombosis in both genders Specific mutations in the factor V (Leiden),
factor II (prothrombin), and methylenetetrahydrofolate reductase (MTHFR)
genes are associated with increased risk for venous thrombosis and
cardiovascular diseases. Furthermore, women undergoing assisted
reproductive procedures, such as in vitro fertilization (IVF) and
intracytoplasmic sperm injection (ICSI), fail to achieve pregnancy in
approximately 70% of cases. Among the possible causes of failure of
embryo implantation might be an impairment of the uteroplacental
circulation due to hypercoagulability in the mother. Several studies have shown an association
between inherited thrombophilias and recurrent early pregnancy loss. The
precise mechanism by which thrombophilias affect recurrent pregnancy
loss and implantation failure is as yet undetermined. Several studies
have reported an association between hereditary thrombophilias and
increased complications of pregnancy, such as severe pre-eclampsia,
fetal growth restriction, stillbirth and abruption of placenta, which
showed an association between recurrent first trimester loss and factor
V Leiden.
Related tests
MTHFR (C677T) mutation analysis MTHFR is a gene involved in the process of DNA synthesis and methylation. The MTHFR 677TT genotype may be a genetic risk factor for male infertility, especially with severe oligo-asthenozoospermia and non-obstructive azoospermia in unexplained infertile males. The C667T in the MTHFR gene decreases the activity of the enzyme by 35% in persons who are heterozygous and by 70% in those who are homozygous. The prevalence of the homozygous form is estimated to be between 5 and 10% in the population. One study showed an increase in sperm count and motility after three months of treatment with folic acid. By determining MTHFR C677T mutation, it may be possible to identify patients who have tendency toward an altered folic acid metabolism and might benefit from folic acid supplementation.
Related test
Y microdeletions Analysis The long arm of the human Y chromosome is required for male fertility. Microdeletions in three different regions can cause severe spermatogenic defects ranging from oligozoospermia to non-obstructive azoospermia. Clinical studies of oligozoospermic and azoospermic patients have shown that Y-chromosome microdeletions can be transmitted to the male offspring after ICSI. Y microdeletions can also affect ICSI efficacy. In a study by van Golde et al. reporting on eight men with AZFc microdeletions and oligozoospermia, fertilization rate during ICSI was statistically lower compared with a control group of oligozoospermic men with intact Y-chromosomes (55 versus 71%, respectively). Furthermore, embryo quality was significantly poorer among the group of Y-deleted men. There are findings suggesting that there might be a potential risk for male offspring, born to fathers with Y microdeletions to develop sex chromosome aneuploidy. This risk is difficult to quantify since it would include not only 45X/46XY individuals but also patients with 45X/Turner syndrome. Furthermore, although individuals with 45X/46XY chromosome complement can develop a wide spectrum of phenotypes, including Turner syndrome, mixed gonadal dysgenesis, male pseudohermaphrodism, mild mental retardation and autism, others are phenotypically normal men. Presence of a 45X/46XY karyotype in a fetus does not predict the sverity of the phenotype. To quantify the potential risk is recommended preimplantation diagnosis when used sperm for ICSI from men with Y microdeletions, to avoid the transfer of 45X embryos. In recent literature, the occurrence of microdeletions varies between 1 and 55% in the heterogeneous group of infertile men and Y microdeletion test should be applied in all men with:
1. Idiopatic (unexplained) oligospermia
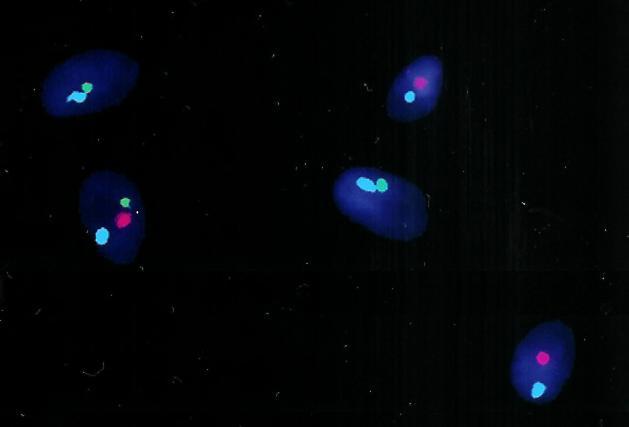
Studies have shown that men with abnormal semen quality generally have an increased rate of sperm chromosome aneuploidy. Aneuploidy and chromosomal aberrations can cause major morphological and biochemical defects in offspring. On the other hand, studies confirm that a normal karyotype does not exclude the presence of chromosomal abnormalities in spermatozoa in male partners of couples with recurrent pregnant loses and normal seminal parameters. Most aneuploidy is attributed to errors in meiotic chromosome segregation during meiosis resulting in aneuploid gametes. Those data are especially pronounced in men undergoing intacytoplasmatic sperm injection because of severely decreased sperm quality. Chromosome defects are a frequent cause of spontaneous abortions, and it is therefore likely that increased gamete aneuploidy could be a cause of some cases of recurrent pregnancy loss. Using fluorescent in situ hybridisation (FISH) a large number of spermatozoa can be analyzed and even spermatozoa of infertile men that are non capable of fertilizing an egg can be scored.
|
BioGenetics © 2006-2013 |